
Robotic Prostatectomy
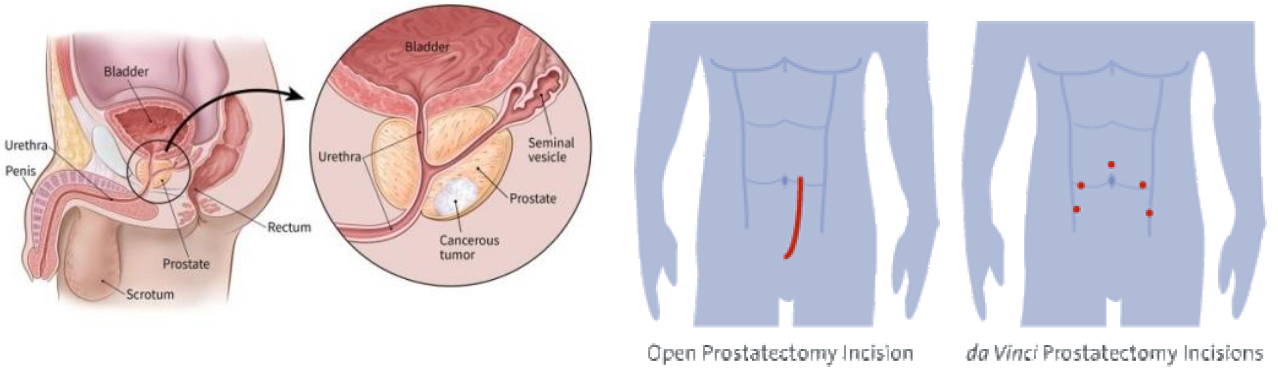
Radical prostatectomy is the removal of the whole prostate containing the cancer to achieve the best possible cure and prevent the cancer from spreading. The da Vinci robot is ideal for this surgery due to the 3-dimensional, 10 times magnified view and small, dextrous instruments that can get right down to the tight pelvic space. The surgeon is able to remove the whole prostate with less damage to the nerves for erection and sphincter for urinary continence. Robotic method gives faster recovery with less pain and minimal bleeding. The surgery is best done after 1 month post-biopsy to allow for the post-biopsy rectal adhesions to settle.
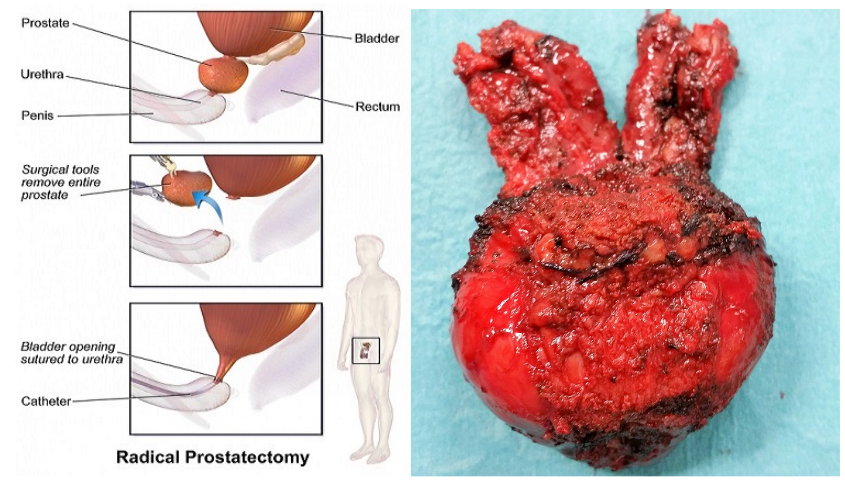
The whole prostate is detached from the bladder and urethra
How it is done
Under general anaesthesia, the abdomen is distended with gas and the robotic ports inserted under direct vision. A total of 6 incisions are made. The patient is then placed in a steep head-down position (about 30 degrees) and the robot docked. The bladder is first taken down to expose the prostate. The prostate gland is detached from the bladder together with its vas and seminal vesicles. The nerves for erection are spared where possible. Finally, the prostate is detached from the urethra without damaging the sphincter muscles. The bladder is then re-joined to the urethra in a watertight fashion over a catheter. The prostate is put in a plastic bag and retrieved from the umbilical incision. The surgery takes between 2 to 3 hours. Hospital stay is 3 days on average.

Patient in steep head-down position

Robotic arms in position
Bladder re-joined to the urethra after prostate is removed
The catheter is removed 1 week later in the clinic as long as the urine is clear yellow. There is no need for a cystogram xray to see if there is any leak.

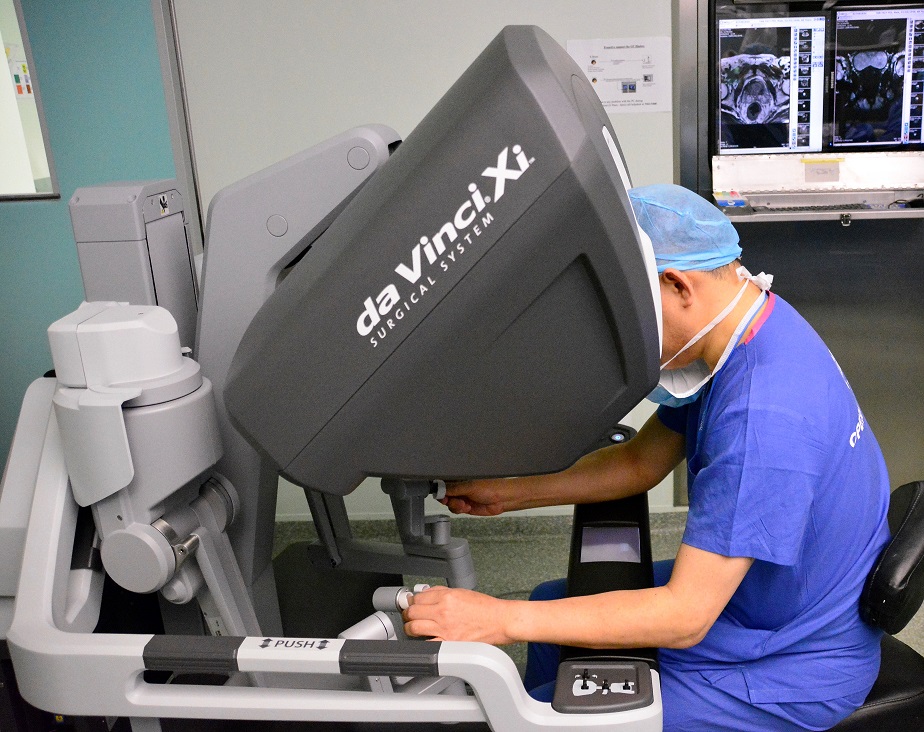
Dr Chin with the latest da Vinci Xi robot
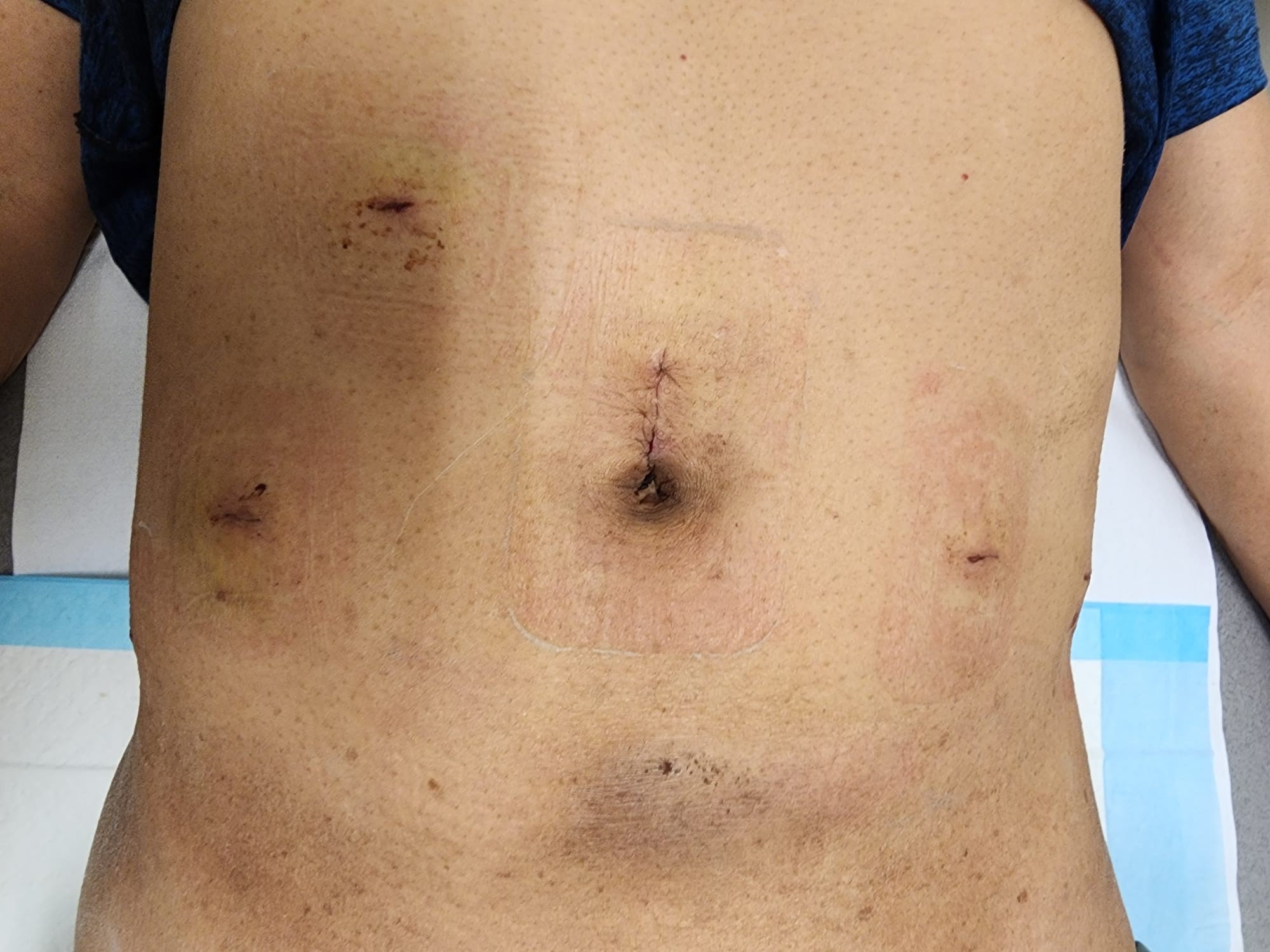
6 small scars after robotic prostatectomy
Watch video on Robotic Prostatectomy
Complications include:
- urine leak. This occurs if the bladder-urethra stitching is not water-tight
- This is usually < 200 ml
- stress incontinence. This is due to weak pelvic floor muscles / damaged sphincter muscle. This recovers by 3 months in 90% of men
- This is due to nerves to the penis being cut. Erection can take between 6 to 12 months to recover depending on the degree of nerve preservation
- rectal injury. This can occur when dissecting the prostate off the rectum. It is more likely to occur if the post-biopsy adhesions are dense e.g. especially when the biopsy was done less than a month
Desired outcomes:
- negative surgical margins (< 10%)
- no anastomotic leak or late strictures ( < 1% risk )
- no blood transfusion ( < 1% rate )
- no permanent stress incontinence (< 1% occurrence)
- no impotence – this depends on the age of patient and whether both or one nerves are spared
- no rectal injury ( < 0.1% risk)