
Microhaematuria
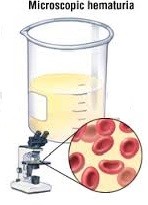

Microscopic haematuria (microhaematuria) is the presence of unseen but significantly high numbers of red blood cells in the urine. It is normal for urine to have very small amounts of blood (< 3 red blood cells per high power field). However if it exceeds 3 red cells, and remains high on repeat testing, it may indicate a kidney disease, stone or a tumour in the urinary system. The white cell count may or may not be high.
Causes
Many people have microhaematuria for many years and yet do not have any identifiable kidney or urinary tract disease. It can also be related to physical exercise or vigorous sports (stress microhaematuria) or hypertension. However, before concluding that such persistent microhaematuria is benign in nature, it is important to exclude any significant urological disease. In order of importance, they are:
- tumours and cancers in kidney or bladder [Fig 1]
- urinary stones [Fig 2]
- kidney parenchymal disease (glomerulonephritis) [Fig 3]
- prostate inflammation (prostatitis) in men [Fig 4]
- bladder inflammation (cystitis) or urethra inflammation (urethritis) in women esp. after menopause [Fig 5]
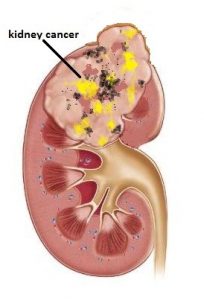
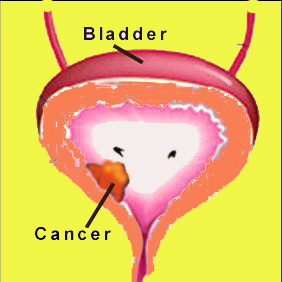
Fig 1. Kidney / bladder cancer
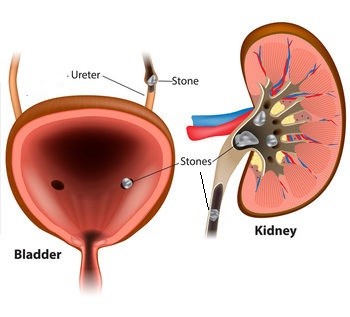
Fig 2. Urinary stones
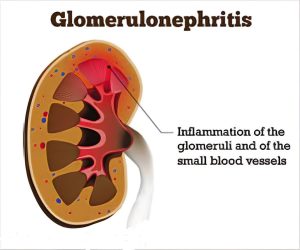
Fig 3. Glomerular disease causes blood to leak out from the kidney
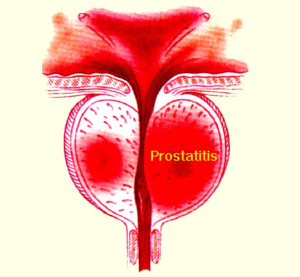
Fig 4. Prostate inflammation
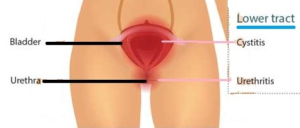
Fig 5. Urethra/ bladder inflammation in women
Investigations
Microhaematuria can only be regarded as idiopathic only after the following investigations have been done:
- urine testsg. phase contrast study to differentiate if the blood is from glomerular disease or urinary tract lining, urine cytology to look for cancers of the urinary tract lining
- radiologic scans, e.g. , Ultrasound, IVU or CT scan
- endoscopy, eg. flexible cystoscopy [Fig 6] which is easily done under local anaesthesia and regarded as the most reliable way of detecting any small tumours / cancer in the bladder. Cystoscopy can also see if the prostate is the source of bleeding
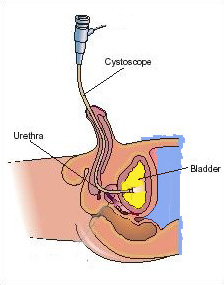
Fig 6. Flexible cystoscopy can easily be done under local anaesthesia
Even if no apparent cause is found after extensive investigations, it is recommended that urine analysis be done at least once a year. This is because kidney stones and tumours may initially be so small that ultrasound or xrays may not show the source. Glomerular disease of the kidney may also not manifest in the initial years.