
Robotic Pyeloplasty
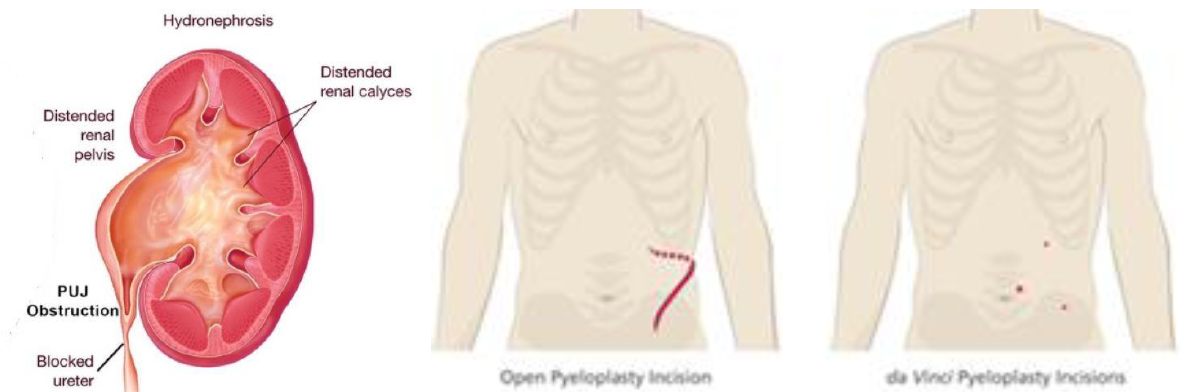
Pyeloplasty is surgery to remove a blockage of the kidney located at the pelvi-ureteric- junction (PUJ). The junction can become narrow due to extrinsic compression by a branch of the renal artery or an intrinsic stricture. The blockage can also be congenitally present at birth. The resultant hydronephrosis can become infected and kidney stones can form. Left untreated, chronic hydronephrosis will eventually lead to deterioration of kidney function and even atrophy of the kidney. The most common early symptom is recurrent pain over the loin, especially after a drinking binge.
Corrective surgery is traditionally done by open method as all types of PUJ obstruction can be managed. Open surgery gives the highest success rate, but leaves a long, painful scar. Laparoscopic surgery gives the same access though small incisions, resulting in less pain, shorter hospital stay, faster recovery and return to daily activities.
Although conventional laparoscopic method can be used, robotic pyeloplasty makes the surgery easier and faster to do. This is due to the increased range of motion of each instrument, Enhanced by magnified visualization on the da Vinci’s 3-D high definition camera, the surgeon can reconstruct the PUJ more precisely with equal success rate to open surgery. In addition, the blood loss is less and recurrence rate is lower compared to laparoscopic method.
How it is done
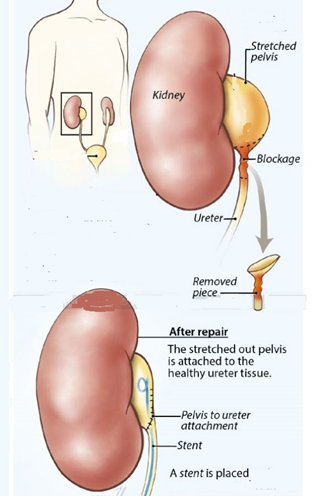
Steps in pyeloplasty
Under general anaesthesia, the patient is placed in a lateral position and all pressure points are padded. The abdomen is distended with gas and robotic ports inserted under direct vision. The kidney and ureter are exposed. The site of obstruction is identified and excised. The baggy kidney pelvis is trimmed and the ureter spatulated prior to being stitched in a water-tight fashion. The surgery takes 2 to 3 hours and a DJ stent is routinely placed to prevent urine leak. The stent is removed 4 weeks later. Hospital stay is 2 days on average.
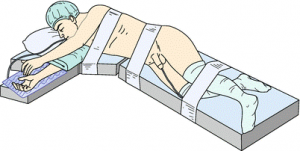
Patient position during robotic pyeloplasty

Robotic arms in position

Dr Chin doing robotic pyeloplasty on the Si robot

Scars after robotic left pyeloplasty in a 103 kg man
Complications include:
- bleeding. If excessive, blood transfusion is given
- urine leak. This occurs if the repair is not water-tight. This will result in fever, pain and bloatedness in the immediate post-op period. The DJ stent prevents such a leak
- conversion. As with all laparoscopic surgeries, conversion to open surgery is always possible if complications occur or the repair cannot be performed. The conversion rate is lower compared to conventional laparoscopy
- recurrence. This occurs if the cause of the obstruction was missed, especially a crossing vessel, if the blood supply of the ureter was compromised or if there was a significant urine leak from imprecise suturing.
Desired outcomes:
- no blood transfusion
- no urine leak ( < 2% risk )
- no conversion to open surgery (< 3% chance)
- no recurrence ( < 1% chance )