
Percutaneous Nephrolithotomy (PCNL)
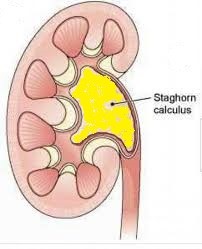

This surgery uses a keyhole approach to break staghorn or large kidney stones > 2 cm size. Shockwave treatment (ESWL) is not suitable because such big stones are not only harder to break, but can also block the ureter when the stone fragments pass down.
How it is done
Under general anaesthesia and xray guidance, a catheter is placed into the kidney via the bladder using a cystoscope. The patient is then turned over to the prone position. Xray dye is injected to outline the kidney system to plan the best approach for the puncture track. A track is established through a series of dilators to allow a nephroscope to be inserted. Through this nephroscope, an ultrasonic, pneumatic probe or laser is used to break the stones and remove the pieces. A nephrostomy tube is left in the kidney at the end of the surgery to drain urine, blood and small stone fragments. This tube is removed after the bleeding has settled.
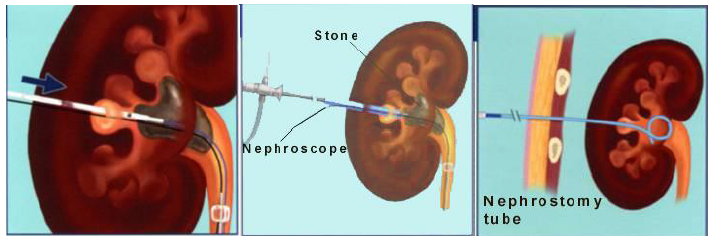
Steps in PCNL surgery
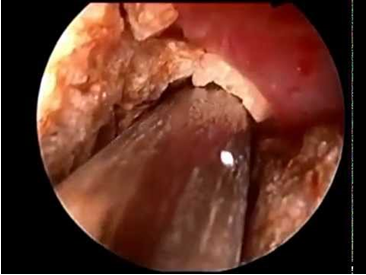
Stone being broken during PCNL

Dr Chin doing PCNL surgery
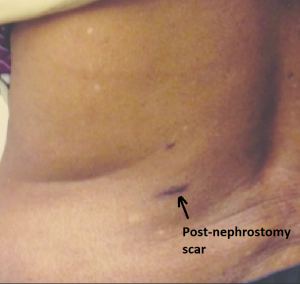
Scar post-PCNL
An xray is done on the 2nd day to look for any significant residual stone fragments. If so, a completion session can be done before removing this tube. Alternatively, this remnant stone can be broken by ESWL. Some leakage of urine can be expected up to 2 days after the nephrostomy tube is removed. The operation takes 2 to 3 hrs and the hospital stay is 3 to 4 days. The success rate (defined as residual fragment < 3 mm) for PCNL is 95%.
Complications include:
- bloody urine. This can last up to 2 weeks. In 3% of cases, an abnormal artery to vein connection (called a-v malformation) can develop to cause re-bleeding. If so, readmission to hospital for urgent radiological embolisation is needed to seal the bleeding vessel
- urine leak. This occurs through the puncture wound at the back. However, it dries up the next few days
- hydrothorax. This rare complication is due to accidental puncture through the lung cavity during the track creation. Chest xray will confirm this and the remedial action is to insert a chest tube for a few days
Desired outcomes:
- no excess bleeding /a-v malformation ( 3% risk )
- no UTI ( 1% risk )
- no large remnant stone needing removal or ESWL ( 5% chance )