
Recurrent Urinary Tract Infection
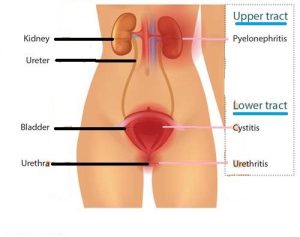
When urinary infection becomes recurrent despite adequate antibiotics and good hygiene practices, an underlying cause should always be suspected.
In Females
Many women suffer from frequent UTIs. About 4 out of 5 women who have a UTI get another in 18 months. It is well known that some women are just more prone to recurrent attacks, especially sexually active women. Post-menopausal women are particularly prone to infection because the cells lining the vagina and urethra lack protective mechanisms, allowing bacteria to attach more easily. Another common reason for recurrent UTI is the persistence of resistant bacteria that were not eradicated the last time round. The widespread use of antibiotics have resulted in resistant strains which remain in the lining of the urethra / bladder. Doctors often give antibiotics based on “best guess” but do not realize that if the bacteria is only partially sensitive to the antibiotics, they can still survive and re-multiple to cause recurrent UTI. Hence, it is important to do a urine culture prior to starting antibiotics to determine if one is dealing with a resistant strain of bacteria [Fig 1].

Fig 1. Urine culture is done to determine which bacteria is causing the infection
Other investigations include ultrasound or xrays of the urinary tract to exclude obstruction, stones or anatomic abnormalities. In women with previous bladder surgeries for incontinence, a cystoscopy may also be needed to exclude any foreign body material.
Women with recurrent UTI with no identifiable cause will benefit from preventive antibiotic therapy. Any woman who has frequent recurrences (3 or more a year) can consider the following treatment options:
- Low dose antibiotic daily for 3 to 6 months, eg. bactrim, nitrofurantoin
- Single dose antibiotic immediately after sexual intercourse
Additional steps that she can take are:
- Drinking plenty of water every day. Drinking cranberry juice may also help because it inhibits the growth of some bacteria by acidifying the urine. Vitamin C supplements have the same effect
- Not holding the bladder for too long because stale urine is a good medium for bacteria
- Passing urine immediately after sexual intercourse
In Males
Recurrent UTI in men are usually related to a long foreskin (phimosis), chronic prostatitis and in men over 50 years, an enlarged prostate (BPH).
A long and tight foreskin tends to trap urine beneath it [Fig 2]. This subsequently allows bacteria to flourish and cause infection of the foreskin (called balanitis) and the urethra to cause UTI. Hence, it is important to practise good penile hygiene to prevent such infections. In those with tight foreskin which cannot be retracted (called phimosis), circumcision surgery will clear the infection.
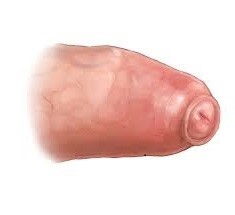
Fig 2. Phimosis or tight foreskin
Young men (20 to 50 years) are also prone to prostate infection (prostatitis). Many of them are assumed to have simple UTI and given a short course of antibiotics which is not sufficient in killing off all the bacteria within the prostate. Chronic prostatitis require at least 3 weeks of antibiotics to completely eradicate the bacteria within the prostate.
Prostatitis can be confirmed through examining the prostate [Fig 3]. In suspected cases of sexually transmitted disease, swab and blood tests are done. Semen can also be sent for culture as it can be hard to determine which type of bacteria is causing the infection.
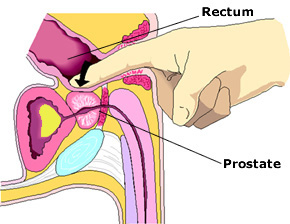
Fig 3. Digital rectal exam of the prostate
Older men with BPH tend to develop stagnant residual urine which subsequently allow bacteria to grow easily [Fig 4]. Treating the UTI is not good enough if the underlying bladder blockage is also not relieved through BPH medication or surgery.
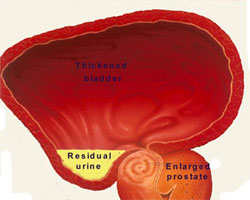
Fig 4. BPH causes bladder blockage leading to residual urine