
Sling Surgery - Tension-Free Vaginal Tape (TVT) or TVT-Obturator
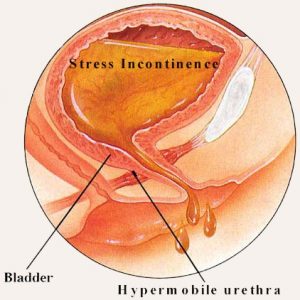
Sling surgery is now the standard procedure to correct stress urinary incontinence in women. It is minimally-invasive with a high success rates (> 95% dry) and minimal complication provided it is done by surgeons trained in continence surgery. This surgery can be done as a day case under general anesthesia.
.
TVT (Tension-Free Vaginal Tape)

TVT inserted under the mid-urethra
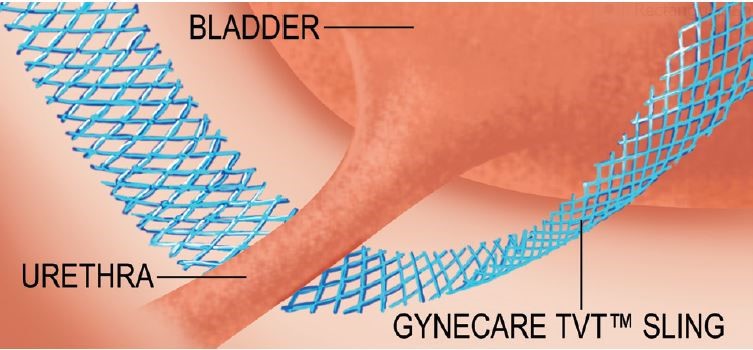
Tape material used in TVT surgery
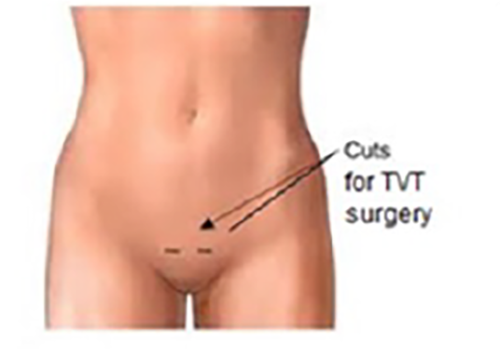
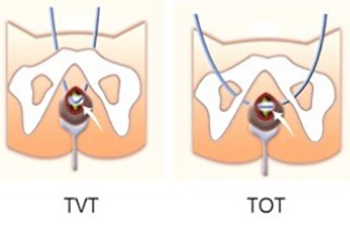
A prolene-material tape is placed under the mid-urethra via a short incision over the vagina and exits through 2 small skin incisions over the suprapubic area. It is then adjusted to a point of minimal leak. The surgery takes 30 to 40 mins to do. It is important to perform a cystoscopy during tape insertion to check for any accidental puncture into the bladder. If tape entry into the bladder is not recognised, this can lead to recurrent bladder infection and stone formation. The cystoscopy also helps the surgeon judge the tape adjustment.

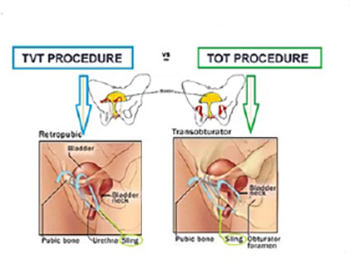
TVT-Obturator or TOT (Trans-Obturator Tape)

A variant of the TVT is the TOT where the tape exits through the inner thigh instead of on top of the pubis. The results are the same, with the advantage of less chance of bladder injury. It is also faster to do but thigh pain can be a consequence as the tape exits through the inner thigh muscle.
Regardless of approach, surgeon training, experience and judgment are still the most important factors for success in any sling surgery.
Complications include:
- bloody urine. This should clear in a few days
- This resolves with time, usually by 2 to 3 weeks
- bladder injury. This occurs during passage of the tape. If so, the catheter has to be kept for a longer period
- difficulty passing urine. This may be due to the tape being too tight. If this does not settle by 2 weeks, the tape will need to be loosened via the vaginal incision
- urgency of urination. This stems from an overactive bladder and seen in 30% of women as the bladder capacity is increased following correction of the stress incontinence. This usually resolves by 1 to 3 months. If not, drugs for overactive bladder can be given
- tape erosion into the vagina or urethra. This is a rare and late complication. The tape will have to be removed if this happens
Desired outcomes:
- minimal haematoma / bleeding
- no bladder injury ( < 8% of cases )
- no urinary retention post-op ( 3% of cases )
- no more stress leak ( > 95% cases )