
Robotic Surgery In Urology

Robotic surgery is the use of robotic technology to perform complex surgeries. This is made possible by the da Vinci Surgical System which comprise of three components: a surgeon’s console, a patient-side robotic cart with 4 arms, and a 10 times magnified, high-definition 3D vision system (Fig 1, 2 & 3). A common misconception is that the robot performs the surgery; the robot is not performing surgery; the surgeon does the surgery using the robot as the interface.

Fig 1. Surgeon console

Fig 2. Robotic arms in position

Fig 3. 3-dimensional vision camera system
Robotic abdominal surgery is an enhancement of standard laparoscopic surgery as the operation is still performed through key-hole incisions in the abdomen. As opposed to standard laparoscopic surgery where hand-held rigid instruments are used, the robotic arms are flexible and mimic the surgeon’s hand and wrist movements, giving greater dexterity, superior strength and better precision (fig 4). These movements are intuitive in nature, i.e. the instrument tips move in the same direction as the human hand and reproduce the same movements as in open surgery. In addition, a filtration feature dampens any hand tremor to improve precision.

Fig 4. The robotic arm mimics human wrist movements
Robotic versus Standard Laparoscopy
Robotic laparoscopy has a shorter learning curve. The combination of 3-D, magnified vision with endowrist, intuitive instrument movements make dissection and suturing so much easier for the surgeon. Although there is no tactile feedback on the robot, this is overcome by the superior vision. In standard laparoscopy, the surgeon has to overcome the limitation of rigid, counter-intuitive instrument movements. He also needs to have a regular, high patient load to maintain his laparoscopic skills. For long laparoscopic procedures, fatigue and muscle ache are bound to set in. On the other hand, the da Vinci robot allows the surgeon to sit comfortably in a chair while doing the surgery. This additional luxury relieves any physical fatigue and allows the surgeon to concentrate better. After all, this is still laparoscopic surgery, just that it is now robotically-assisted.
Advantages of Robotic Surgery
Robotic surgery has been shown to improve patient’s recovery because of:
- Less pain
- Less blood loss
- Less scarring
- Less damage to surrounding structures
- Fewer complications
As a result, hospital stay is shorter and return to regular activities faster.
Application
Robotic surgery is now used in the fields of:
- Urology
- General Surgery
- Cardiac surgery
- Gynaecology
- Head & Neck surgery
For urology, robotic surgery is ideal for:
- Prostate Cancer
- Kidney Cancer
- Kidney pelvis obstruction
- Ureter stricture
- Bladder cancer
- Bladder-Vagina Fistula
Prostate
Radical Prostatectomy
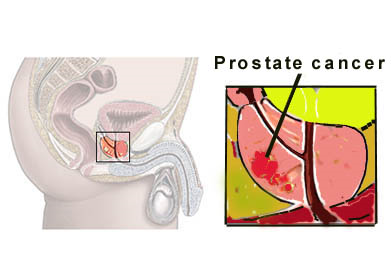
Radical prostatectomy is the removal of the whole cancerous prostate to achieve the highest cure rate. Prostate cancer is most common in Western countries, but it is also rising in Asia due to dietary factors and early detection. Prior to the use of robotic surgery, prostatectomy surgery was done via a long open incision over the lower abdomen (Fig 5). Besides greater wound pain and slower recovery after surgery, the open method carried a high blood loss with blood transfusion rates as high as 67%. With the robotic method, blood loss is minimal, usually less than 200 ml, resulting not only in negligible transfusion rate but also quicker recovery. As of 2020, up to 95% of all radical prostatectomies done in the United States were performed robotically.
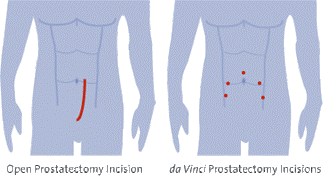
Fig 5. Incisions for open compared to robotic method
Robotic prostatectomy has become the single most popular robotic procedure because the small dextrous robotic arms, together with a magnified 3-D view is ideal for surgery in the narrow male pelvis. After removing the prostate, the bladder needs to be re-joined to the short urethra stump. This is the most difficult part of the surgery, even for the experienced laparoscopic urologist. The robot makes this task easier because the flexible arms make stitching intuitive and precise with the operator comfortably seated. The other concern which many patients have is the functional consequence of incontinence and impotence. Once again, the superior vision of the robotic system helps the surgeon to better identify and preserve the nerves and structures responsible for continence and erection. Many centres are now reporting better cancer clearance and faster recovery of continence and potency compared to open and standard laparoscopy. Robotic prostatectomy is now the new “gold standard” in centres that have the da Vinci robot.
Kidney
a) Pyeloplasty
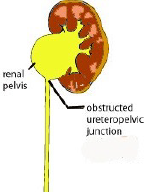
Pyeloplasty is the surgical repair of an obstructed pelvi-ureter junction (PUJO). In this condition, the urine outflow from the kidney is blocked by a narrow junction. This abnormal segment usually needs to be excised and continuity is restored through stitching of the tissue flaps. The standard method is open surgery. Laparoscopic method is also feasible but takes a long time because of the limited stitching ability of the rigid instruments. The robot makes this stitching task easier through the dexterous arms. Centres are now reporting shorter operating times. The overall success rate of > 95% is also identical to open and standard laparoscopic methods.
b) Partial Nephrectomy
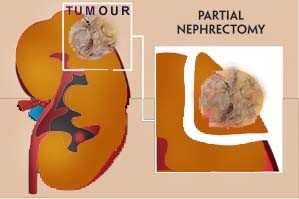
Nephrectomy is the removal of the whole kidney and performed mostly for kidney cancers more than 4 cm in size. In total nephrectomy, there is no suturing involved. Hence, the advantage conferred by the robot is similar to standard open or laparoscopic surgery. However, for smaller tumours < 4 cm, partial nephrectomy is technically possible with the advantage of sparing most of the kidney and thus avoid or delay kidney failure. The disadvantage in partial nephrectomy is that a water-tight closure of the collecting system is crucial to avoid urine leak. The kidney defect also needs to be repaired to avoid excess bleeding. Yet, this whole task has to be done within 30 mins as the kidney can only tolerate a short period of ischaemia. For standard laparoscopy, such a repair is a challenge because stitching is much more difficult to perform. Once again, the robot’s superior suturing capability helps the surgeon to close the defect within this limited time frame.
Ureter
Reimplantation
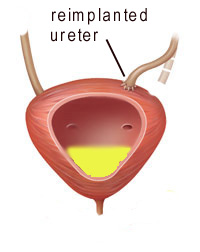
Ureter stricture consequent to injury or inflammation may not always be amenable to endoscopic means. In such a situation, re-implanting the obstructed ureter to another site in the bladder is the only way to relieve the kidney obstruction. Open surgery is the traditional method, but laparoscopic re-implantation is also feasible and avoids a long scar. Once again, the limitation with standard laparoscopic method is the stitching, which is tedious and time-consuming. The robot with its intuitive and dextrous arms makes this task easier with greater precision and water-tightness.
Bladder
a) Radical cystectomy
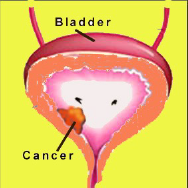
Radical cystectomy is the removal of the entire bladder and this is mostly done for invasive bladder cancer. Open surgery is already a complex and long one fraught with excess bleeding. With the robot, the superior vision and flexible arms makes dissection a less bloody one with the advantage of superior magnified vision of the blood vessels and structures around the bladder. Together with the smaller incisions, recovery is faster and hospital stay shorter. An experienced team is needed for this surgery.
b) Gynae-urology
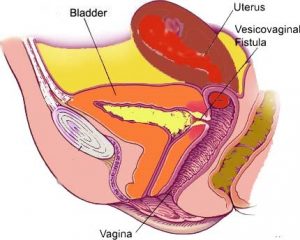
Surgery to correct stress urinary incontinence in women related to fibroids and utero-vaginal prolapse can be done robotically too. Vesico-vaginal fistula can similarly be repaired robotically with the advantage of better visualisation.
The challenge
The robot has made minimally-invasive surgery a safer and technically superior one. Surgeons can now perform more “exacting surgery” thanks to enhanced vision and articulate instruments. The main disadvantage is lack of tactile feedback and the surgeon is remote from the operating table. Hence, it is important to have a regular team of trained assistants and nurses. The robotic surgical system is a high financial outlay; the set-up cost, maintenance cost and training requirements make it difficult for many hospitals to own a da Vinci robot. Nevertheless, the evidence is clear as far as robotic prostatectomy is concerned, as it has the edge over standard laparoscopic and open surgery with superior oncologic, clinical and functional outcomes. Not surprising, there is a trend for patients to travel to leading hospitals that offer robotic prostate surgery despite the higher cost. More countries are now making their own robotic machines and the challenge is how these versions can do the same surgery at a lower cost.
Fig 6. The current da Vinci Xi robot
Figures 3,4, 5 & 6 provided with kind courtesy of Intuitive Surgical, Inc.,California, USA