
Robotic Partial Nephrectomy
Partial Nephrectomy
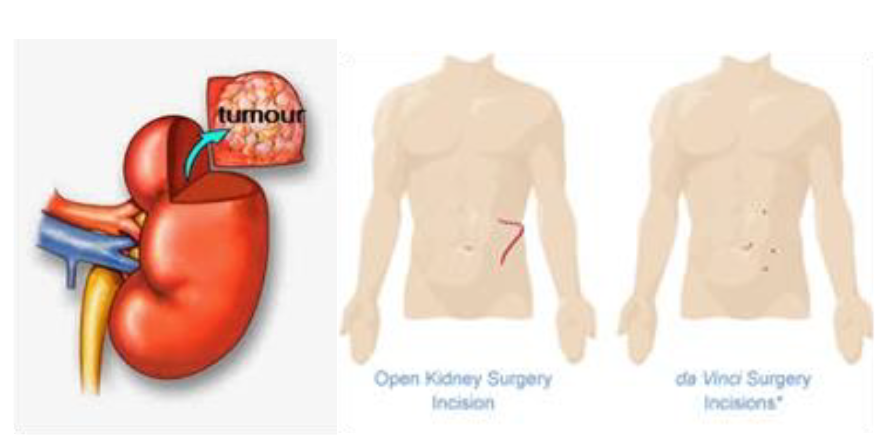
Partial nephrectomy is possible for small kidney tumours of < 4 cm. When done for cancerous tumours, it offers the same cure rate as total nephrectomy while conserving as much normal kidney tissue. The standard method is open surgery but this would result in long scar, prolonged wound pain, numbness, longer recovery period and permanent muscle bulge. Standard laparoscopy avoids these complications but is technically more difficult to perform, and carries a higher chance of conversion to open surgery if there is excess bleeding and if the kidney defect cannot be repaired. Robotic method gives the benefit of faster, more precise and water-tight repair of the kidney defect with lower chance of conversion to open surgery.
In partial nephrectomy, the blood flow to the kidney has to be interrupted. However, it is imperative to limit this time to a minimum as kidney function deteriorates quickly after 30 minutes of ischaemia. The robotic system allows the surgeon to reduce the surgery time, thanks to the superior vision, dexterity and precision of the instruments. It is important to stitch the bleeding vessels to minimise the blood loss, and close the defect in a water-tight fashion to control any urine leak.
Robotic partial nephrectomy requires special instruments, e.g. laparoscopic ultrasound probe, robotic bulldog clamps, barbed sutures and a highly specialized team.
How it is done
Under general anaesthesia, the patient is placed in a lateral position and all pressure points padded. The abdomen is distended with gas and the robotic ports are inserted under direct vision. The robot is docked from the side. The whole kidney has to be exposed and its main blood vessels dissected carefully and individually separated. The tumour is located with the laparoscopic ultrasound probe. The tumour margins are marked and the arteries to the kidney are occluded with bulldog clamps. After the tumour is excised, the defect is repaired in 2 layers using sutures. Upon completion, the bulldog clamps are then removed and any bleeding areas stitched or sealed with coagulant glue. The tumour is placed in a plastic bag and extracted out via one of the ports at the end of the surgery. The surgery takes 3 to 4 hours. Blood loss is 300 – 500 ml on average. Hospital stay is usually 4 days.
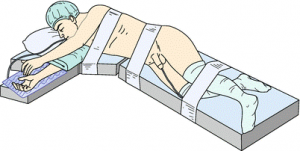
Patient position for robotic kidney surgery

Robotic arms in position
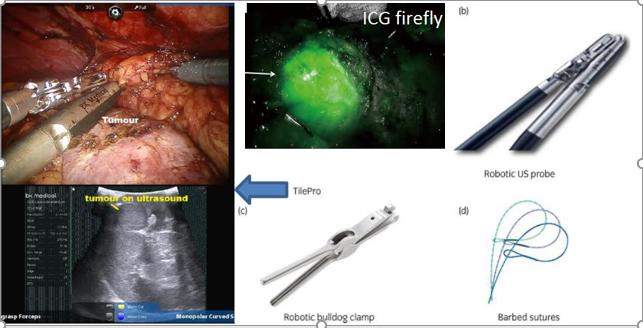
Laparoscopic ultrasound for locating the tumour & other requirements for robotic partial nephrectomy
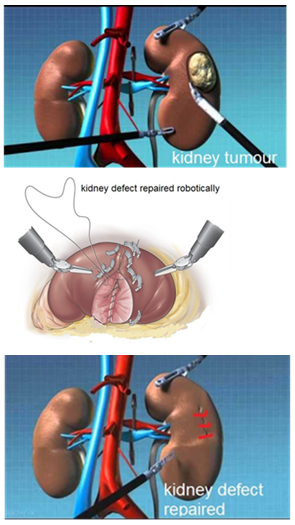
Steps in partial nephrectomy
Dr Chin performing robotic partial nephrectomy on the latest Xi robot
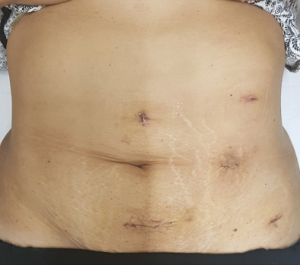
Scars from robotic left partial nephrectomy for a 7 cm kidney tumour in a 55 year old woman
Watch video on Robotic Partial Nephrectomy
Complications include:
- bleeding. Blood loss is generally limited (< 300 ml) but blood transfusion may still be needed if the bleeding is excessive. In desperate situations, the whole kidney may have to be removed.
- urine leak. This occurs if the kidney defect is not repaired in a water-tight fashion. This will result in fever, pain and bloatedness in the immediate post-op period. If the urine leak is excessive, a double-J stent may need to be inserted.
- conversion. As with all laparoscopic techniques, conversion to open surgery is always possible if any difficulty is encountered or if the bleeding cannot be controlled
- remnant tumour. Cancerous tissue can be left behind if the tumour is violated during its excision. The histology will report a ‘positive margin’. If so, the chance of recurrent cancer is high and total nephrectomy is recommended.
- kidney atrophy. This occurs if the ischaemic time goes beyond 45 mins.
Desired outcomes:
- no blood transfusion (up to 20% of cases )
- no urine leak ( < 5% risk )
- no conversion to total nephrectomy ( 5 to 10 % chance )
- no conversion to open surgery (< 10% chance)
- ischaemia time < 25 mins
- no positive margins / recurrence of tumour ( 3% chance )